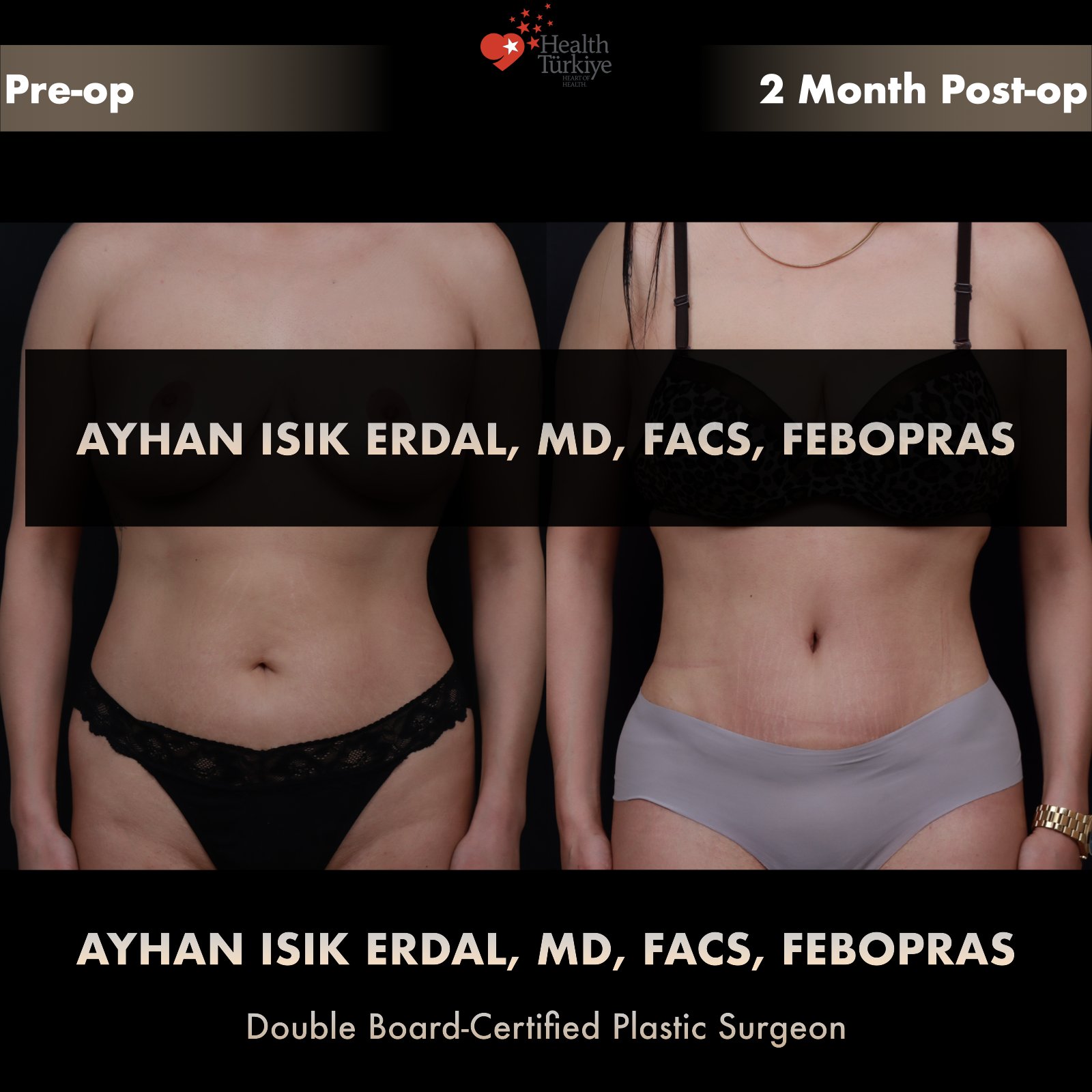
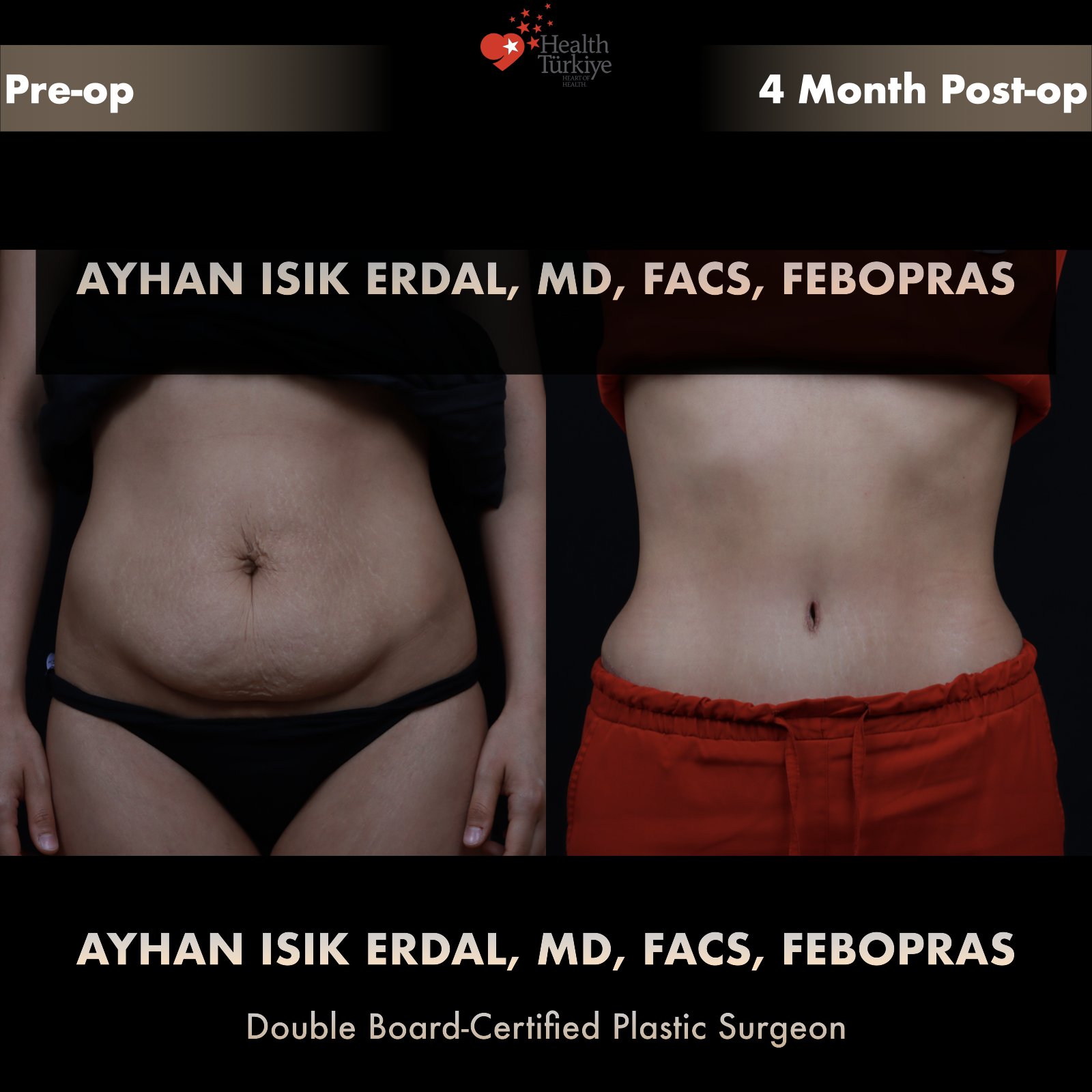
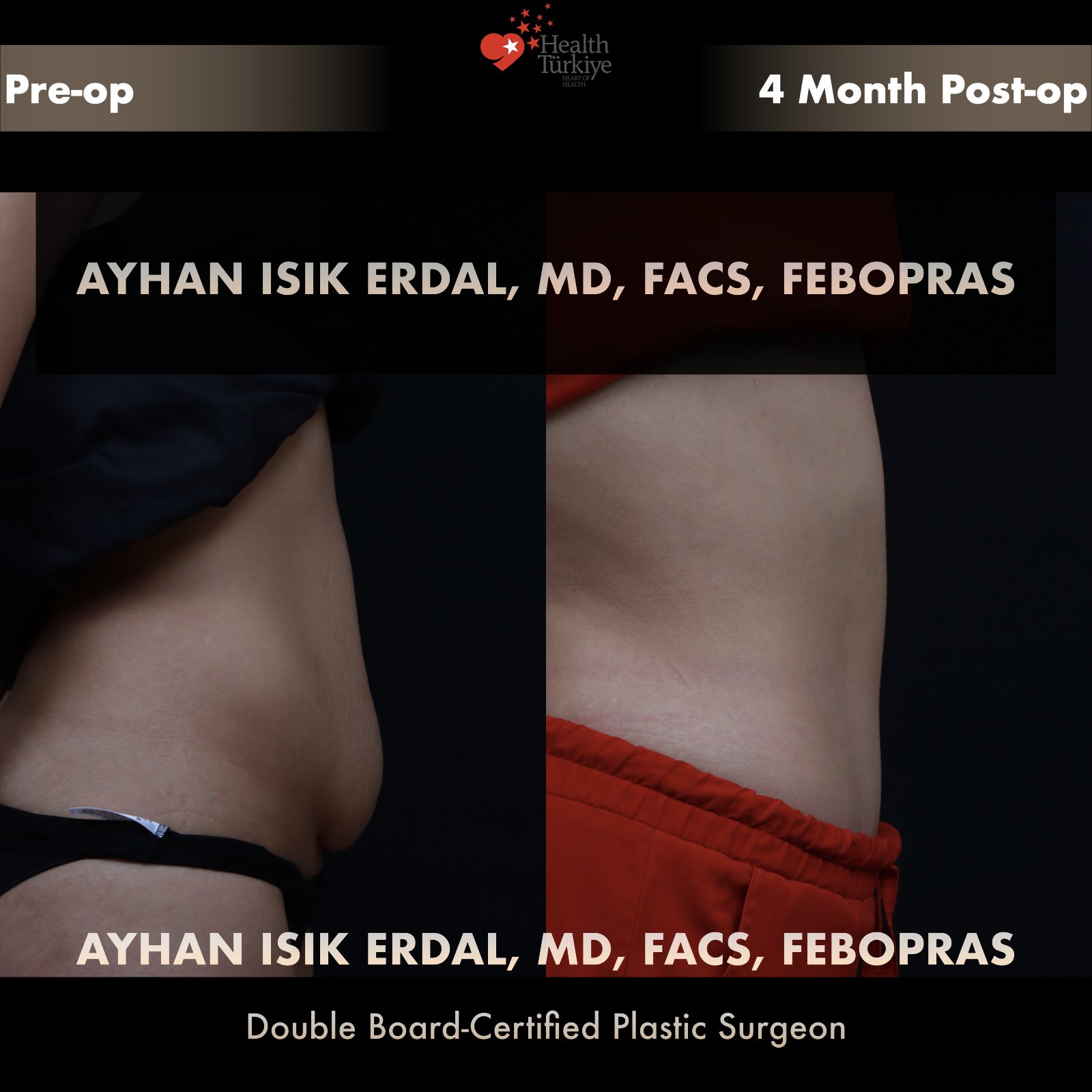
Istanbul · Abdominoplasty & Body Contouring
Technique-driven abdominoplasty — tailored to anatomy, not to price.
Assoc. Prof. Dr. Ayhan Işık Erdal — double board-certified plastic surgeon, Associate Professor with 30+ peer-reviewed publications and international fellowship training. Extended, fleur-de-lis and lipoabdominoplasty with Scarpa-fascia preservation, perforator-sparing dissection and progressive-tension closure.
Fellow · FACS
American College of Surgeons · 2025